
Chapter 1: How do 340B programs work?
When a patient receives a 340B-eligible prescription from an eligible entity, the entity is reimbursed for the full market price of the drugs, but pays only a fraction of the drugs’ cost — by replenishing the medication from the 340B catalog.
Who pays the 340B costs?
Manufacturers bear the burden of the cost and reimburse wholesalers for 340B discounts on 340B-eligible medications.
How does the 340B payment process work?
As a covered entity, you send your encounter (visit) data to your TPA, and your pharmacy sends the TPA the prescription data. Your TPA creates a match when it determines that 340B qualification criteria has been met, and your pharmacy then orders from your 340B account to replenish the drugs.
Clients served by VytlOne use a proprietary software system, which monitors every prescription their organizations fill, and identifies every eligible prescription generating sufficient savings to justify the time and effort to claim 340B savings. This extra layer of monitoring improves compliance, while hunting-down hidden opportunities for more 340B savings.
VytlOne works with each client to determine how aggressively they want to pursue 340B savings. We then maintain comprehensive records on every prescription applied for — always assuring clients of complete compliance.
Which pharmacies can I use for 340B prescriptions?
340B-eligible hospitals can use the in-house (or on-campus) retail pharmacies they own and manage, as well as “contract pharmacies” — which can be both on-campus and off.
You can extend 340B eligibility to contract pharmacies (onsite or off) if they meet HRSA’s requirements — which include the following: Your contract pharmacies must 1) register for the 340B Program, 2) be listed on the 340B OPAIS prior to dispensing 340B drugs on your behalf, 3) not use 340B drugs for Medicaid patients unless you have an arrangement in place with the state.
Covered entities often choose contract pharmacies to dispense 340B drugs to patients for a number of reasons. Many hospitals, for instance, prefer their on-campus retail pharmacies to be operated independently. Some hospitals reach contract pharmacy agreements with multiple pharmacies in their communities, offering their patients more convenience, access and options when filling prescriptions written by their providers.
SIMPLIFIED PAYMENT PROCESS*
(No Manufacturer Restrictions)
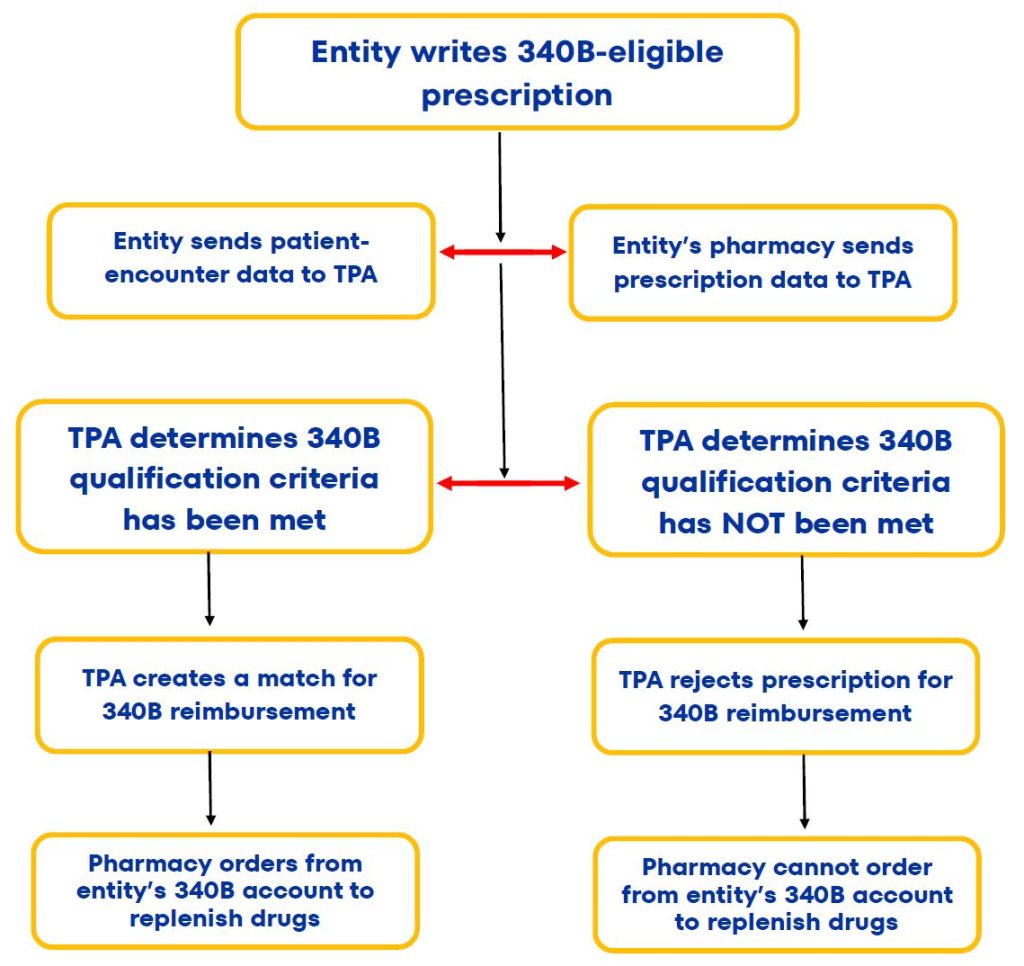
*NOTE
The TPA steps described above are for off-site contract pharmacies, but aren't necessary for health systems' on-campus pharmacies.


What Are The Requirements For 340B Programs?
Covered entities must meet the following ongoing requirements:
- Keep 340B OPAIS information accurate and up to date.
- Register new outpatient facilities and contract pharmacies as they are added.
- Prevent diversion to ineligible patients.
- Maintain auditable records documenting compliance with 340B Program requirements.
As a covered entity, it’s also your responsibility to notify drug manufacturers and wholesalers that you plan to purchase drugs at 340B prices. The wholesalers and manufacturers verify your enrollment on the 340B database and must sell their drugs to you — at or below the maximum price determined under the 340B statute.
How do I enroll in the 340B program?
To register, you need a 340B Office of Pharmacy Affairs (340B OPAIS) user account. To get started, visit the 340B OPAIS Registration page, and select the appropriate link toward the bottom of the page — either Grantee Registration or Hospital Registration.
The system should run you through the process from there. It’s important to know, in advance, that you must complete your registration in a single session. Which is why you’ll need to have your latest filed Medicare cost report on-hand while you’re completing the process.
You’ll also you’ll need to enroll your main location first, then add any Child Sites.
What is a 340B Child Site?
HRSA defines a 340B Child Site as an off-site outpatient clinic or location that uses, or purchases, 340B drugs for its patients. In general, “off-site” means a location has a separate physical address than the hospital parent site, and is not located within the main hospital.
The following types of facilities are included in the 340B program
- Freestanding acute care general hospitals
- Psychiatric hospitals
- Long term/continuing care nursing homes
- Home infusion therapy centers
- Hospices
- Federally qualified health centers
- Rural health clinics
- State mental institutions
- Indian Health Service facilities
- Federally Qualified Health Centers
- Community-based rehabilitation programs.


Which patients are covered under 340B programs?
Covered entities can dispense 340B-eligible prescriptions to patients who (1) Have established relationships with the covered entity, such that the entity maintains records of the patient's care; (2) Receive care from a professional employed by the covered entity, or under contract or other arrangements (e.g., referral for consultation) with the covered entity, such that responsibility for the care remains with the covered entity; and (3) Receive health services from the covered entity that are consistent with the services for which grant funding has been provided to the entity.
Under these guidelines, an individual is not considered a covered entity’s patient if the only health care service received by the patient from the entity is the dispensing of a drug for subsequent self-administration — or administration in the home setting.
Are 340B prices available for inpatient prescriptions?
No. 340B pricing applies to covered outpatient prescriptions only. Covered entities must therefore maintain appropriate tracking systems to ensure that covered outpatient drugs purchased through the 340B Program are not used for hospital inpatients — and it is the responsibility of health systems in the program to ensure that appropriate safeguards are in place to prevent these diversions.
What prescription drugs are eligible for 340B Savings?
In general, 340B eligibility involves both prescription medications and the covered entity writing the prescriptions. Here’s a simple checklist for determining whether drugs are eligible.
- As a covered entity, you have a relationship with the patient and maintains records of care.
- The services are provided by a healthcare professional who is either employed by, or contracted with, you.
- The responsibility for care rests with you, the covered entity.
- The services are within the scope of project for grantees and designees.
- The service provided must be more than just dispensing medication.
- The drug is administered in an eligible outpatient location or dispensed by one of your 340B contract pharmacies.
General drug exceptions to 340B eligibility
There are a few 340B-eligibility exceptions. These include vaccines and Orphan Drugs (which are, by definition, medications specifically developed to treat rare diseases or conditions — and drugs that have only recently been granted New Drug Status by the FDA).
Eligible drugs frequently NOT submitted for 340B savings
While narcotic medications are included among 340B eligible drugs, covered entities often choose to exclude them from their programs — due, primarily, to the complexity of procuring these medications for replenishment. That procurement complexity adds-up to significant time-and-effort costs. And as we’ve noted in a previous post, there’s no point in utilizing 340B discounts for medications when the time-and-effort costs exceed the savings generated.
About 340B Orphan Drugs
For the following covered entities, 340B-covered drugs do not include any drugs designated by the Secretary under Section 526 of the Federal Food, Drug, and Cosmetic Act for rare diseases and conditions:
- Free-standing cancer hospitals
- Rural referral centers
- Sole community hospitals
- Critical access hospitals
Take full advantage of specialty drug discounts
Specialty drugs, which Medicare defined (in 2019) as any drug costing more than $670 monthly, constituted about 50% of the overall prescription drug market’s expenditures (some $161 billion) in 2020. That’s a 29% increase of total expenditures over 2015. What’s more, according to Acentrus Specialty, 8 out of every 10 new drugs approved by the FDA in 2020 were specialty drugs. All of which makes specialty drugs the fastest-growing, and largest part, of the prescription-drug market.
Specialty pharmacies generate fewer 340B-eligible claims, and higher net savings
According to the estimates of several online sources, the average retail pharmacy prescription in 2020 cost $566 per month — while the average specialty drug prescription cost $6,565. AARP estimated, in a September 2021 article, that —in 2020 — the average annual cost for a single specialty medication used on a chronic basis was $84,442.
340B exposure risk is decreased.
Fewer claims means less exposure to potential audits and compliance claims. What’s more, most specialty pharmacies have dozens, even hundreds, of 340B contract pharmacy relationships; which means that they’re highly experienced, and educated, in maintaining 340B compliance for the covered entities they serve.

Implement a robust Meds To Beds program
Benefits of a Meds To Beds Program: Overview
On a purely practical level, a well-managed bedside prescription delivery program can improve your health system’s pharmacy revenue.
On the human level, Meds To Beds is more than a tangible sign of your system’s care of, and for, the individuals & families you treat. It’s your first line of offense in ensuring that your patients follow the prescription protocols you’ve given them — significantly decreasing the likelihood of their readmission while, in the process, improving your patient’s satisfaction ratings.
In general, health systems fail to implement Bedside Prescription Delivery programs because of the costs of staffing and administrations. In our experience, managing dozens of Meds to Beds programs, those costs are more than offset by the revenues generated. In one Mississippi health system alone, VytlOne filled over 18,000 outpatient prescriptions in just 12 months. During that time, the health system’s pharmacy revenues increased 125%, while its readmissions decreased 79%.
How a good Meds To Beds Program works
First, your health system’s retail pharmacy staff must commit to partner with your case management teams, nurses and physicians to implement a cohesive medication treatment plan for your patients who are transitioning back to their lives at home. That commitment means your pharmacy staff must be willing to perform the work necessary to enhance your health system’s current efforts, ensuring that there is never any additional burden placed on your hospital’s providers, nurses and staff.
Next, when prescriptions are delivered bedside to discharging patients, you should be sure to have a pharmacist available to help patients —reviewing both prescription protocols and any issues that could compromise your patients’ willingness (or ability) to maintain compliance with their prescriptions after they leave the hospital.
Once a patients accepts his or her prescriptions, and understands how to maintain compliance, your meds to beds program should pass-off the job of continued patient contact to a readmission risk reduction program.
How Meds To Beds benefit 340B drug programs
Bedside prescription delivery is arguably the most effective method for ensuring that your patients’ prescriptions are captured before they leave your care.
Put another way, your Meds To Beds program should not only support health systems' mission of maximizing patient care, compliance and satisfaction while minimizing readmissions, it should serve as a funnel for directing patients into 340B programs. This role is particularly significant, when you consider the aggressive efforts manufacturers have undertaken to minimize the number of pharmacies that 340B-eligible hospitals can utilize in their 340B programs.
Many manufacturers have launched initiatives to limit their support of eligible entities’ contract pharmacies to one per hospital. They’ve also fought HRSA’s efforts to overturn those limits, through protracted legal battles. It goes without saying, those manufacturers have determined that legal battles are less costly to them than upholding their legal obligation to support 340B drug discounting.
How Meds To Beds benefits your 340B patients
Patients entered into your 340B program “funnel” generally receive superior ongoing professional care and support, after they are discharges. And as we’ve mentioned elsewhere, hospitals with multiple contract pharmacies in their networks offer patients more choices, and convenience, in filling their prescriptions.
Statistical research conclusively demonstrates that two primary factors driving patient non-compliance are lack of education and understanding, and lack of access (both in terms of financial means and proximity) to pharmacies. Which is why many hospitals with 340B programs supplement their Meds To Beds programs by offering home delivery and prescription discounts to financially-challenged patients. Those health systems generally agree that the costs of additional patient support are more than offset by the benefits of superior post-discharge care — not to mention the savings that come with reducing readmissions.
According to a 2020 study published by Frontiers In Public Health, Meds To Beds programs have been shown to significantly reduce 30-day hospital readmissions — particularly among older adult patients.
VytlOne’s Impact© Readmission Reduction Program
In late 2023, VytlOne took all the fundamental components of its Meds To Beds programs, and developed a 30-day readmission reduction program we call Impact®.
Using a clinical pharmacist in collaboration with a health system’s nursing team, the program emphasizes personal, one-on-one patient education and medication-compliance support. The program operates as a separate service from Meds To Beds prescription delivery, but it can easily work in collaboration with MTB. All that’s needed to add Impact® to a Meds To Beds program is an onsite clinical pharmacist and a virtual team of nursing care coordinators.
As we reported in a blog post detailing the program’s initial implementation (at South Carolina’s Conway Medical Center), when our program launched in November, 2023, CMC’s health system had a baseline 47% readmission rate among MVP patients with three or more encounters. After 15 months, our program had enrolled and served 474 participants — and achieved a readmission rate of just 10.1%. Of those patients, past the 30 day mark, 379 patients “graduated” without readmission — and there were only 48 readmits, for an 88.5% graduation rate. Readmissions dropped 77% among patients with 3 or more encounters, and 93% among patients with uncontrolled A1C.
The savings CMC achieved in readmission avoidance costs, as a result of the program, was $1.25 million (based on the $15,200 readmission cost per patient cited above). What’s more, patient satisfaction ratings with the program (142 survey respondents) was 9.77 out of 10 — nearly 50% higher than the national average of 6.6 for health system Hospital Consumer Assessment of Healthcare Providers and Systems Survey (HCAHPS) scores.
To read the full blog post (which includes a video), click the link below:
How To Achieve Readmission Reduction, One Patient At A Time
To read a profile of the program’s Clinical Pharmacist, Click Here.

Understand, and overcome, your TPAs’ limitations
TPAs play a critical role in 340B programs. It’s their job to “match” prescription claims from your contract pharmacies with patient data hospitals provide, and then to determine the eligibility of those claims. Without a match, a prescription cannot be qualified for 340B eligibility and savings.
Your TPAs’ ability to accurately qualify your 340B claims is only as reliable as the information you provide. Their systems simply aren’t configured to monitor and spot mismatches in that data.
340B data mismatches can be extremely trivial.
One of the most common reasons 340B claims are misqualified — particularly with Medicare patients — is inconsistency in Date Of Birth entries. Patient Name mismatches is another common cause of misqualifications. For instance, you may have a patient registered as Bob in your pharmacy system and Robert on your hospital’s system.
That said, the more complex 340B programs are, the higher the likelihood that their automated data submission process will be flawed. Which will naturally lead to missing EHR encounters and missed 340B savings opportunities — quite possibly substantial savings opportunities.
Technology often causes 340B data mismatches
The process of monitoring 340B programs is especially difficult when multiple TPAs are involved. Every TPA’s proprietary software system’s interface is unique. Making matters even more complicated, the reporting structure within TPA portals vary significantly from one to another. We’ve found that health system 340B personnel often spend an inordinate amount of time simply trying to access the information that they need — which leaves them far too little time to proactively take advantage of that information.
How common are TPA 340B misqualifications?
Mismatch rates vary from health system to health system, but we can say this with confidence: If you have a 340B program already in place, it’s probably a lot higher than you think.
One of the health systems VytlOne serves employs three experienced and well-trained full-time professionals — who monitor their system’s 340B claims on a full-time basis. And yet, during the first six weeks VytlOne supported their efforts, we provided matching justification for, and generated $187,000 worth of, 340B savings that they’d overlooked.